A Historic First for Endometriosis
How 2026 Federal Report Language Changes the Future of Research and Care
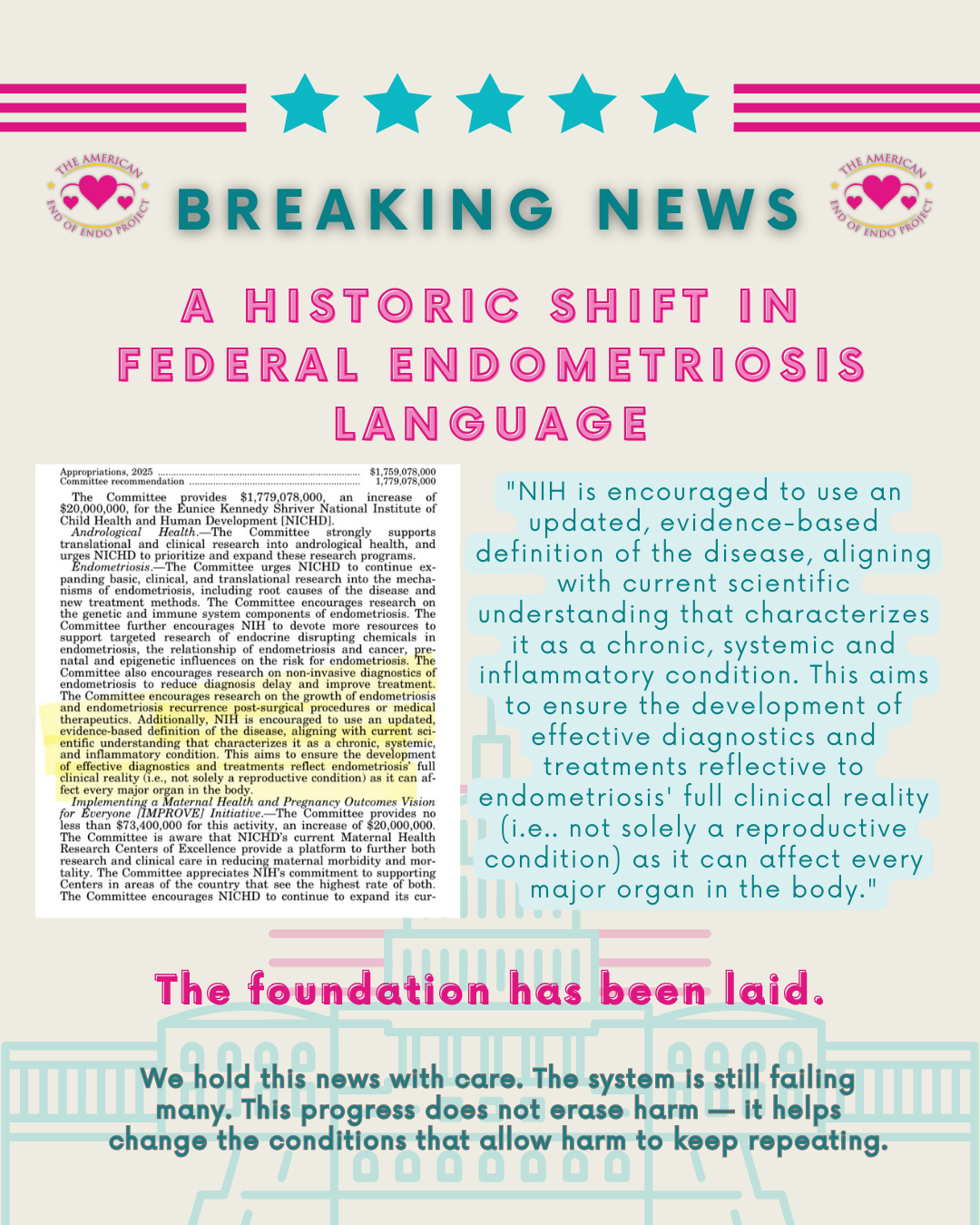
For the first time in United States history, federal appropriations report language has formally recognized endometriosis as a whole body, chronic, systemic, inflammatory disease.
This congressional report language was driven by the American End of Endo Project (AEEP) through sustained, patient-led education and coalition-based advocacy. AEEP worked directly with congressional appropriations offices to provide evidence-based education on the systemic nature of endometriosis, centering patient lived experience alongside clinical research and emerging scientific data.
The language was formally introduced by Senator James Lankford (R) of Oklahoma, with engagement and support from offices across party lines, including Senators Lindsey Graham (R), Bill Cassidy (R), Chris Murphy (D), John Boozman (R), and Lisa Blunt Rochester (D). This bipartisan engagement was made possible by framing endometriosis as a public health issue rooted in evidence, disability impact, and systemic harm rather than a narrowly defined or partisan concern.
This work focused on correcting a long-standing misclassification of the disease, reframing endometriosis beyond a reproductive-only lens, and ensuring federal research language reflected the full clinical reality patients have documented for generations.
While this recognition appears in the report language accompanying the Fiscal Year 2026 appropriations process rather than as standalone legislation, its impact is structural. Appropriations report language is one of the most powerful tools Congress has to guide federal agencies. It shapes definitions, priorities, and accountability, and agencies rely on this language to maintain eligibility for current and future funding.
This is how systems begin to move.
A Disease Trapped in History
Nearly 2,500 years have passed since the earliest recorded observations of symptoms we now associate with endometriosis. References to wandering womb theories can be traced back to ancient Egyptian medical texts and carried forward through Greek and Roman medicine into the third and fourth centuries. These early frameworks falsely linked women’s suffering to social roles, suggesting that if a woman failed to fulfill expectations of marriage or motherhood, her uterus was deprived of purpose and would cause illness.
It is difficult to comprehend that echoes of these beliefs persisted for centuries and, in many ways, still shape modern medical thinking. While the language has changed over time, the consequences of framing a complex disease through a narrow reproductive lens have remained.
The first microscopic identification of lesions occurred in 1860, when Karl von Rokitansky documented abnormal tissue growth, though the disease had not yet been named. In 1925, John Sampson formally described endometriosis and proposed the retrograde menstruation theory. While foundational, this theory ultimately reinforced again the uterine-centered framework that would dominate research for an entire century.
From the 1930s through the 1990s, discovery was largely left in translation. Endometriosis remained narrowly defined as “displaced uterine lining tissue”, despite mounting clinical observations that contradicted this simplification. During this period, the disease was routinely minimized, misunderstood, and underfunded.
Modern advocacy began to emerge in the late twentieth and early twenty-first centuries:
1993 – The first Endometriosis Awareness Week launched
2000s – Awareness efforts expanded globally, centering March as an international advocacy month
2009 – The U.S. Congressional Endometriosis Caucus was established, providing patients an entry point into legislative dialogue
2010s – The NIH began shifting public-facing definitions toward tissue “similar to” the uterine lining, reflecting incremental scientific progress
2014 – Worldwide EndoMarch coordinated the first synchronized global marches across more than 40 countries
2019 – New York became the first U.S. state to mandate menstrual health and endometriosis education in schools
2020 – Federal funding for endometriosis research at the NIH was doubled
2022 – The Endometriosis CARE Act (H.R. 7974) was introduced
These milestones mattered. They raised awareness, expanded dialogue, and created visibility. But awareness alone did not dismantle the structural misclassification at the heart of the problem.
That is why February 2026 marks a historic arch in the timeline.
For the first time in United States history, federal appropriations report language encourages the NIH to use an updated, evidence-based definition of endometriosis, aligning with current scientific understanding that characterizes it as a chronic, systemic, inflammatory, whole body disease capable of affecting multiple organs throughout the body.
This is not a symbolic acknowledgment. It is a course correction that was centuries in the making.
What took millennia to mis-define will not be fixed overnight.
This moment represents the beginning of movement out of historical quicksand and into a future where science is finally allowed to follow reality. 2026 is not the end of this timeline, it is the opening of a new chapter.
Why Definitions Matter
For decades, endometriosis has been framed narrowly, often confined to a reproductive or women’s health category that failed to reflect clinical reality. Patients have long known what science increasingly supports. Endometriosis is not limited to the uterus. It is not limited to the pelvis. It is not limited to one phase of life.
It is a systemic disease that can involve multiple organs, systems, immune pathways, inflammatory responses, neurological mechanisms, and long-term health outcomes. When a disease is misunderstood at the federal level, everything downstream is affected. Research questions are narrow. Diagnostic pathways stall. Training pipelines remain incomplete. Treatment options lag behind need.
By recognizing endometriosis as chronic, systemic, and inflammatory, federal report language now aligns more closely with lived experience and scientific evidence. Definitions determine outcomes. When the definition changes, everything that follows becomes possible.
A Structural Shift Inside the NIH Research Ecosystem
Following sustained federal advocacy and direct collaboration with congressional appropriations staff, new FY26 federal research report language has been adopted that explicitly restructures how endometriosis is positioned within the National Institutes of Health research ecosystem.
Rather than confining endometriosis research strictly under the umbrella of women's health initiatives, the placement of this language under general NIH and NICHD guidance broadens the scope in which endometriosis research can be considered. While this shift may appear technical on paper, its implications are significant. Research classification determines which scientific questions can be asked, which institutes can lead investigations, and which expertise is brought to the table.
This restructuring opens doors to multi-organ, immune, inflammatory, and neurological research pathways that were previously difficult to access. It also allows pediatric and adolescent research pipelines to expand, reflecting the long-established reality that endometriosis often begins years, sometimes decades, before diagnosis.
By aligning federal research architecture with clinical and lived evidence, this language creates the conditions necessary for more accurate science, earlier intervention, and better long-term outcomes.
Funding Was Protected, Not Lost
At the same time, overall NIH research funding has been protected in the newly released federal funding bill. In a fiscal climate where many anticipated deep reductions, baseline research capacity has been maintained and modestly increased in key areas, while high-risk innovation pathways such as ARPA-H also continue to be supported.
This matters because structural recognition without research capacity would be hollow. In this case, funding has not been lost. Research capacity has not been reduced. Instead, endometriosis has been repositioned within a research ecosystem that remains active, funded, and capable of growth.
Structural Reform Versus Awareness
This moment illustrates the difference between symbolic awareness and structural reform. Awareness campaigns ask institutions to care. Structural policy tells institutions how to classify disease, where to invest, and which priorities guide decision-making.
For the first time in federal policy history, endometriosis is being recognized within research architecture as a systemic disease. That recognition influences how grants are reviewed, how training programs are developed, how interdisciplinary teams are formed, and how future innovation is funded. It also signals to scientists outside traditional gynecology that endometriosis belongs in their field of inquiry. When disease definitions expand, scientific responsibility expands with them.
A Public Health Issue With Bipartisan Support
Framing endometriosis as a public health issue was essential to this progress. This framing allowed conversations to move beyond gendered assumptions and into population-level impact. Chronic pain, delayed diagnosis, loss of workforce participation, mental health consequences, and disability are not niche concerns. They are public health realities.
Approaching endometriosis through this lens opened doors across party lines and demonstrated that addressing the disease is not partisan. It is practical. It is necessary. It is humane. It affected their constituents across the board.
Patient advocates met with elected officials to share evidence, lived experience, and clinical realities so policymakers could make better decisions for their constituents. This work followed nonprofit compliance standards and mirrored the principles taught through advocacy workshops across the country. This moment proves that grassroots, patient-led education can shape federal policy, even within systems that often feel inaccessible.
When people understand how systems work, they can change them. This recognition was shaped by people who are living with chronic illness. Advocates navigating surgery recovery, mobility limitations, and complex disease still showed up. One advocate entered the Senate building in a wheelchair just two weeks post-operation. Others balanced recovery from Lyme disease, CRPS, and preparing for cross-country surgery. Their presence carried a clear message.

Aubrey Svensson (Left), Holly Sanneman (Center Left), Chelsea Hardesty (Center Right), & Hannah Foerster (Right) stand in front of the Nations Capitol in D.C March 2025 after meeting with 25 congressional staff offices. This was not their first trip, but the one that stuck with staff members.
Being sick does not disqualify someone from leadership. This work challenges the idea that only the healthy, wealthy, or well-connected can shape policy. It proves that bottom-up change is still possible. Behind every policy shift lies human stories.
Years spent searching for answers, stories of symptoms dismissed. Of lives interrupted. Of resilience that should never have been required. By sharing these stories alongside data, advocates reframed endometriosis as a condition with real consequences, not abstract statistics. Storytelling became a tool for truth, accountability, and hope.
Anonymous was a woman, and she has never been invisible.
Clarifying Endometriosis and Adenomyosis
This shift also clarifies long-standing confusion between endometriosis and adenomyosis. While the two conditions can coexist and are often discussed together, they are not the same disease.
Adenomyosis is a reproductive organ disease confined to uterine tissue, characterized by endometrial-like tissue growing into the uterine wall. Endometriosis, by contrast, has been documented in pulmonary regions, thoracic cavities, vascular structures, and non-reproductive organ sites. It has been identified in animals and in men, including cases unrelated to exogenous hormone exposure.
These differences are not academic. They determine which organs are studied, which specialists are involved, and how care pathways are designed.
Perhaps in the future, adenomyosis will receive its own dedicated reproductive research focus. It deserves that attention. But endometriosis has now begun to step beyond a reproductive-only box and into the full biomedical research landscape where it belongs.
That is how true progress in healthcare begins. Not with slogans or outrage-driven narratives, but with infrastructure, collaboration, inclusion, and care.
This Is Just the Beginning
This moment is a milestone, not a conclusion. Through patient-led work, coalition-building, and sustained education, the American End of Endo Project helped lay the groundwork for this shift. The recognition now embedded in federal research language belongs to a broader community that refused erasure.
To the patients who documented harm.
To the advocates who showed up while unwell.
To the families who demanded better futures.
The foundation has been laid. What comes next depends on how this moment is protected, expanded, and carried forward.
The ground has been broken and a foundation is laid.
Let’s keep building.